Protocols/Consent Form
Thermal Imaging Protocols and Consent Form
General:
1. You cannot be sunburned or have a fever when you come for the thermogram.
2. Please do not wear deodorant or an anti-perspirant.
3. Please inform us if you have had radiation treatment within the last 6 months.
4. Please do not apply creams, lotions, talcum powder or skin products to/on your upper torso, including your Face.
5. NO FRAGRANCES APPLIED ANYWHERE ON BODY.
6. NO TANNING BEDS.
Twenty-Four (24) hours prior to your Thermogram:
1. Please do not use analgesic creams, balms, magnets or poultices.
2. Please do not shave under your arms.
Forty-Eight (48) hours prior to your Thermogram:
1. Please do not have chiropractic care, acupuncture, physical therapy, massage therapy or dental work before
you arrive.
2. No PEMF, BEMER, ALPHA-STEM or any other type of electrotherapies.
Four (4) hours prior to your Thermogram:
1. Please do not have a hot shower.
2. Please do not use seat warmer in your car.
3. Please do not consume caffeine (coffee, tea, chocolate).
4. Please do not consume/use nicotine.
5. Please do not exercise.
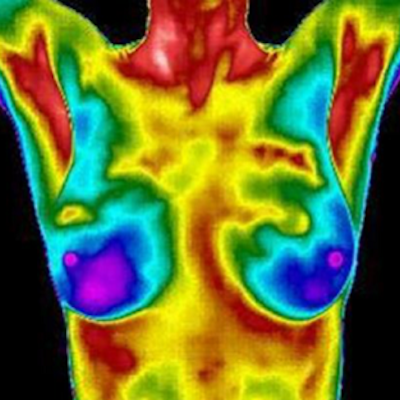
Thermography of the breasts is a procedure utilizing a computerized thermal imaging camera to visualize and obtain an image of the heat coming from the surface of the skin. The thermographic procedure is performed to evaluate/interpret any temperature patterns of the breasts which may or may not indicate the presence of disease in progress.
Thermography is NOT a stand-alone screening. It is adjunctive and should be used by a physician or health care practitioner along with other tests and procedures. No surgical procedure should be based on breast thermal imaging alone. Physical examination, mammography, ultrasound, palpation, MRI, biopsy, blood test, etc. may be needed.
I understand that I will be disrobed from the waist up to allow the surface of my body to cool to an ambient room temperature. This procedure does not use radiation or compression, and it has no known risks or side effects.
The information provided will be made available to my physician or other health care practitioners for evaluation of my breast health. I have been given preparation protocols to insure the most accurate thermographic evaluation of my breasts possible and I agree that I have completed the requirements.
I certify that I have complied with the above protocols and/or I have noted (with NO after the protocol) any protocol(s) with which I was unable to comply. Based on the number of protocols with which I was unable to comply, a decision can be made about needing to reschedule the thermogram.
I understand that Breast Thermography is a Risk Assessment Tool used in evaluating breast health and is not a stand-alone screening.
With my signature below, I consent to having the Breast Thermogram.