If you are not currently on Birth Control, or Hormones, what is your history of Birth Control or Hormone Replacement?
Have you noticed any change(s) in your breasts? Check below all that apply:
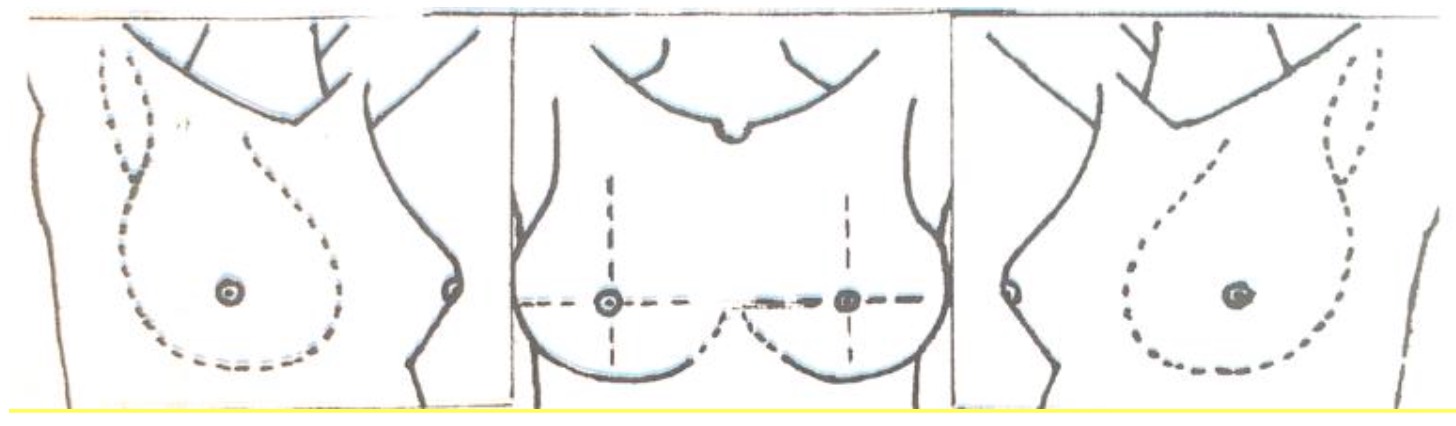
Please describe from the diagram below where you have anything noteworthy (past or present), such as locations of cysts or cyst aspirations, biopsies, surgeries, skin problems, infections, calcifications, etc.
Please indicate below the procedures you have had and dates of these procedures: